1. Invests in the acquisition of evidence through participation in workshops, continued education and pursuit of additional degrees.
During my time at my first level II fieldwork rotation, I participated in many inservice opportunities, one of which being about the Bioness H200 Hand Rehabilitation System. This device looks somewhat similar to a hand splint, but it is an electrical stimulation device that is used for clients with lower arm weakness following injury or disease of the brain or spinal cord. We tried on the device to understand how it can assist individuals with functional hand movements like reaching, grasping, opening, and closing the hand. All of these prepare individuals to be able to engage in more high-level tasks. Each device is programmed to the individual to provide stimulation to the appropriate nerves and muscles. This was such a unique experience with a device that I had never gotten to use before!
During my time at my first level II fieldwork rotation, I participated in many inservice opportunities, one of which being about the Bioness H200 Hand Rehabilitation System. This device looks somewhat similar to a hand splint, but it is an electrical stimulation device that is used for clients with lower arm weakness following injury or disease of the brain or spinal cord. We tried on the device to understand how it can assist individuals with functional hand movements like reaching, grasping, opening, and closing the hand. All of these prepare individuals to be able to engage in more high-level tasks. Each device is programmed to the individual to provide stimulation to the appropriate nerves and muscles. This was such a unique experience with a device that I had never gotten to use before!
2. Is a knowledgeable consumer of global research related to occupational therapy and utilizes an evidence based approach to practice.
I frequently utilized evidence-based resources to assist me in my learning experiences throughout both level II rotations. There were a few diagnoses that I came across during my second level II rotation being in a children's hospital with so many clients going in and out. For the diagnoses that I was unfamiliar with, I made sure to research those to gain a good understanding of the diagnoses and evidence-based interventions to assist with my treatment planning. One diagnosis that was very common during my second level II fieldwork was hypoplastic left heart syndrome, which is a congenital heart defect that affects normal blood flow through the heart. Many of my clients on the cardiac floor were there to receive at least one of the three surgeries that are performed for hypoplastic left heart syndrome. My fieldwork educator encouraged me to have a thorough understanding of this diagnoses as it was one that was very common within my setting, so I made sure to research what the diagnoses was, what each surgery entailed, and how I needed to alter my treatment plans when working with these clients. One example of how I altered my treatment plans when working with a client with hypoplastic left heart syndrome was when I came up with a plan but then began to chart review and noticed that the client was scheduled for surgery. The doctors strongly encouraged clients who were status post cardiac surgery to be up and moving as soon as possible, but I had to first make sure the client was awake, extubated, and cleared for therapy. Once I arrived to my client's room, I altered my plans from more strenuous activities to simpler activities. We got out of bed to ambulate as far as possible around the cardiac floor while being on monitors and then completed oral care at the sink while taking rest breaks when needed.
I frequently utilized evidence-based resources to assist me in my learning experiences throughout both level II rotations. There were a few diagnoses that I came across during my second level II rotation being in a children's hospital with so many clients going in and out. For the diagnoses that I was unfamiliar with, I made sure to research those to gain a good understanding of the diagnoses and evidence-based interventions to assist with my treatment planning. One diagnosis that was very common during my second level II fieldwork was hypoplastic left heart syndrome, which is a congenital heart defect that affects normal blood flow through the heart. Many of my clients on the cardiac floor were there to receive at least one of the three surgeries that are performed for hypoplastic left heart syndrome. My fieldwork educator encouraged me to have a thorough understanding of this diagnoses as it was one that was very common within my setting, so I made sure to research what the diagnoses was, what each surgery entailed, and how I needed to alter my treatment plans when working with these clients. One example of how I altered my treatment plans when working with a client with hypoplastic left heart syndrome was when I came up with a plan but then began to chart review and noticed that the client was scheduled for surgery. The doctors strongly encouraged clients who were status post cardiac surgery to be up and moving as soon as possible, but I had to first make sure the client was awake, extubated, and cleared for therapy. Once I arrived to my client's room, I altered my plans from more strenuous activities to simpler activities. We got out of bed to ambulate as far as possible around the cardiac floor while being on monitors and then completed oral care at the sink while taking rest breaks when needed.
3. Integrates individual clinical expertise and patient values with the best available external clinical evidence.
During all of my fieldwork experiences, I always used what I learned in the classroom as a foundation to my clinical practice. One important topic that was proven to be very beneficial during my first level II rotation was about fall prevention and home modifications. In inpatient rehab, most of my clients were over 60 years old, and they required safety training for fall prevention, as well as recommendations for home modifications following discharge. I had never had much experience working with older adults up until that point, so I heavily relied on lectures from my didactic portion of school and research that I did on my own. Some things I recommended were adding grab bars and railings in showers, using adaptive bathing equipment, removing clutter in the house, and ensuring that areas in the home were well lit during mobility to prevent risk of falls in the dark. I was able to confidently provide the best recommendations for clients and their families following discharge so that my clients could increase safety and independence at home.
During all of my fieldwork experiences, I always used what I learned in the classroom as a foundation to my clinical practice. One important topic that was proven to be very beneficial during my first level II rotation was about fall prevention and home modifications. In inpatient rehab, most of my clients were over 60 years old, and they required safety training for fall prevention, as well as recommendations for home modifications following discharge. I had never had much experience working with older adults up until that point, so I heavily relied on lectures from my didactic portion of school and research that I did on my own. Some things I recommended were adding grab bars and railings in showers, using adaptive bathing equipment, removing clutter in the house, and ensuring that areas in the home were well lit during mobility to prevent risk of falls in the dark. I was able to confidently provide the best recommendations for clients and their families following discharge so that my clients could increase safety and independence at home.
4. Applies the domain of occupational therapy in gathering, evaluating, setting goals, planning and implementing occupational therapy.
Throughout both of my level II rotations, I always worked to ensure that I was taking a holistic approach with my care. When first meeting clients and their families, I conducted a thorough occupational profile to determine that client's values, beliefs, occupations, etc. Knowing these specific things aided my treatment planning to ensure I was focusing on meaningful occupations while also providing engaging activities. The domain of occupational therapy has a common foundation which then branches out to create different methods of planning, evaluating, and treating based on the setting. Below is a comment from one of my fieldwork educators where I received an exemplary performance rating regarding my understanding of the role of occupational therapy and the ability to effectively communicate that to others:
Throughout both of my level II rotations, I always worked to ensure that I was taking a holistic approach with my care. When first meeting clients and their families, I conducted a thorough occupational profile to determine that client's values, beliefs, occupations, etc. Knowing these specific things aided my treatment planning to ensure I was focusing on meaningful occupations while also providing engaging activities. The domain of occupational therapy has a common foundation which then branches out to create different methods of planning, evaluating, and treating based on the setting. Below is a comment from one of my fieldwork educators where I received an exemplary performance rating regarding my understanding of the role of occupational therapy and the ability to effectively communicate that to others:
5. Contributes to the knowledge base of OT practice by mentoring students, performing research, publishing, presenting and/or teaching.
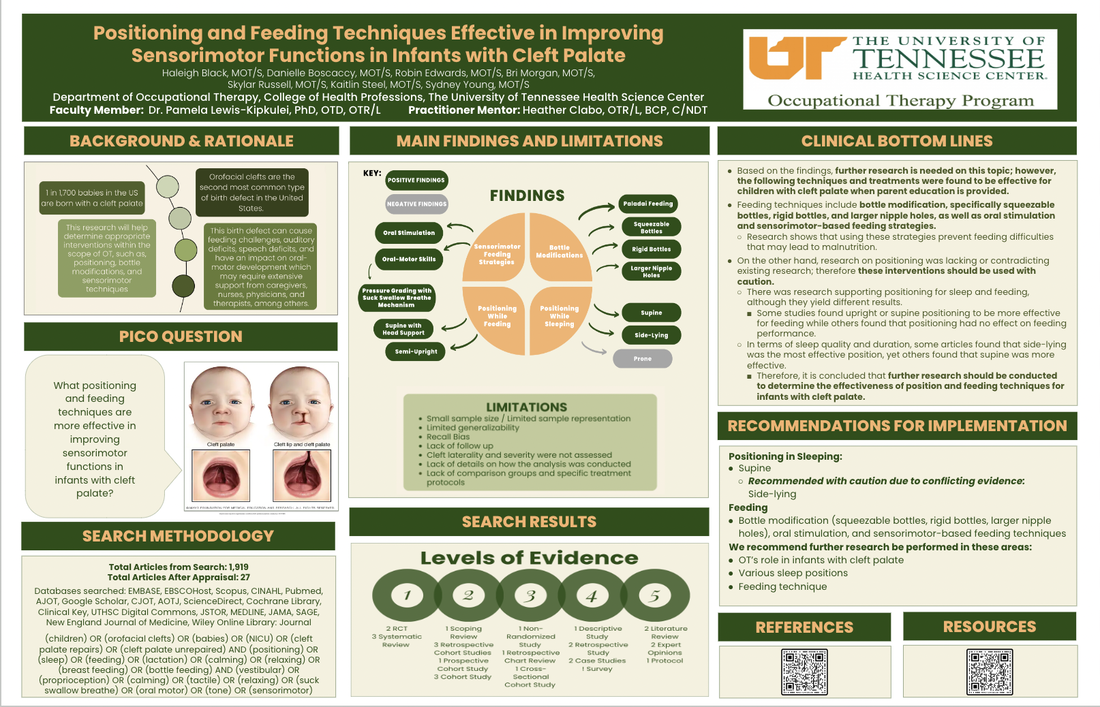
One of the most influential moments during my time in OT school where I contributed to the knowledge base of OT practice partnering with a community OT to participate in research for our final EBP class. Six of my classmates and I conducted research on feeding and positioning techniques for infants with cleft palate (see poster below). We partnered with an OT from LeBonheur Children's Hospital to answer the research question "What positioning and feeding techniques are effective in improving sensorimotor functions in infants with cleft palate?" Through this research, we were able to discover the unique contributions that OTs can provide for feeding when working with infants with cleft palate as LeBonheur Children's Hospital was interested in opening up a cleft clinic where they needed to determine an OT's role in that setting.
One of the most influential moments during my time in OT school where I contributed to the knowledge base of OT practice partnering with a community OT to participate in research for our final EBP class. Six of my classmates and I conducted research on feeding and positioning techniques for infants with cleft palate (see poster below). We partnered with an OT from LeBonheur Children's Hospital to answer the research question "What positioning and feeding techniques are effective in improving sensorimotor functions in infants with cleft palate?" Through this research, we were able to discover the unique contributions that OTs can provide for feeding when working with infants with cleft palate as LeBonheur Children's Hospital was interested in opening up a cleft clinic where they needed to determine an OT's role in that setting.
6. Incorporates continued education as a lifelong practice with the commitment to remain up-to-date and well-informed.
I completed a continuing education course on brachial plexus injuries prior to completing my level II fieldwork in a children's hospital to prepare myself for the possibility of working with infants who have experienced this type of injury. The brachial plexus is complex, so understanding my role when working with infants who have experienced brachial plexus injuries was something that intrigued me. I learned about the different types of injuries, evaluation and treatment methods, and important guidelines that follow surgical procedures. There is always more learning to do, so I plan to continue to expand my knowledge and skills by taking continuing education courses as much as possible over the span of my career. Below is a copy of my certificate following completion of the course:
I completed a continuing education course on brachial plexus injuries prior to completing my level II fieldwork in a children's hospital to prepare myself for the possibility of working with infants who have experienced this type of injury. The brachial plexus is complex, so understanding my role when working with infants who have experienced brachial plexus injuries was something that intrigued me. I learned about the different types of injuries, evaluation and treatment methods, and important guidelines that follow surgical procedures. There is always more learning to do, so I plan to continue to expand my knowledge and skills by taking continuing education courses as much as possible over the span of my career. Below is a copy of my certificate following completion of the course: